Hodgkin’s Lymphoma / Disease
History
This was discovered by Sir Thomas Hodgkin in 1832. But nobody gave any attention to this discovery.
Wilks rediscovered in 1856 this disease and gave his name.
Jackson and Parker divided Hodgkin’s disease in 1944 into :
- Paragranuloma
- Granuloma
- Sarcoma
Luke’s et al gave another classification in 1966 which correlate with prognosis.
Criteria for Hodgkin’s Lymphoma:
- This is a morphologically distinct variety.
- It always arises in lymph nodes.
- There is a contiguous spread.
- There is no leukemic phase.
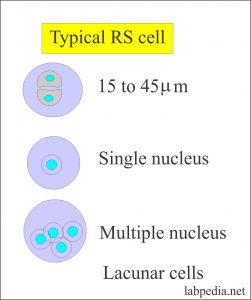
- There are typical cells called Reed Sternberg cells.
- It has an inflammatory infiltrate.
- Atypical Variant of Reed Sternberg cells are:
- Cells with a single nucleus.
- Cells with multiple nuclei.
- There are cells with lacunar nuclei.
- Reed Sternberg cells are also found in:
- Mycosis fungoides.
- Soft tissue sarcoma.
- Infectious mononucleosis.
- Lymphoma.
- Solid carcinoma.
Reed Sternberg cell Origin
There is a suggestion for the origin of Reed Sternberg cells from B cell or T cell or Histiocytes.
- B – lymphocytes marker are seen as Ig, Kappa, and lambda, CD19, and CD20 positive.
- T – lymphocyte markers are also seen as CD 3, CD 5 CD 2 and TCR /
 .
. - Histiocytes cells markers are also present.
- So general consensus is origin from lymphocyte which may be activated B or T lymphocyte.
- Origin from the mononuclear phagocytic cells is not accepted.
 Inflammatory cells accumulate due to the production of cytokines by the Reed Sternberg cells.
Inflammatory cells accumulate due to the production of cytokines by the Reed Sternberg cells.
Other cytokines detected are :
- IL 4, IL 5, TNF-
 , GM-CSF, TGF- β.
, GM-CSF, TGF- β. - IL -5 Correlates with increased eosinophils infiltrate.
- TGF- β is a fibrogenic cytokine found in the nodular sclerosis type.
Incidence
- This disease can be seen at any age.
- There are two peaks.
- There are rare before the age of 2 years.
- These are common after the age of 10 years.
- This disease is more common in males.
- The male to female ratio is 2:1 to 3:1.
- Nodular sclerosis type has an equal male to female ratio.
- 0.7% are all new cases of cancer in the USA (roughly 74000 / year).
Etiology
- This exactly not known.
- This was presumed as inflammatory onset and infection.
- There is a different mode of presentation in different countries.
- In the USA a smaller peak is 15 to 34 years and the larger peak is in older patients (50 years and above).
- This disease is rare in Japan.
- This is more common in male children of the underdeveloped countries. Some believe it that this transmission of infection.
- Report of Albany school, New York showed more incidence of this disease in that school.
- There are reports of familial outbreaks.
- T – cell dysfunction:
- Where Kaplan extracted immunosuppressive factors from these patients.
- There is a cutaneous anergy.
- More chances to develop an opportunistic infection.
- Viral hypothesis. EBV virus found in the late stage.
- EBV- DNA found in some cases.
Classification of Hodgkin’s Lymphoma
Jackson and Parker classified in 1944
- Paragranuloma
- Granuloma
- Sarcoma
Luke’s et al classified in 1965 which was based on Lymphocytes and histiocytes.
- Diffuse lymphocyte-predominant
- Diffuse histiocyte predominant
- Nodular lymphocyte-predominant
- Nodular histiocyte predominant
- Nodular sclerosis
- Diffuse fibrosis
- Reticular type
Rye Classification 1965
- This is dependant upon:
- The number of Reed Sternberg cells.
- A number of lymphocytes.
- The host response :
- Hodgkin’s lymphocytic predominant 10%
- Hodgkin’s lymphocytic depletion 10%
- Hodgkin’s mixed cell type 20%
- Nodular sclerosis 60%
Sign and Symptom
- Stage 1 and 11 may be symptoms free.
- Due to obscure or unknown mechanism, there may be :
- Weight loss.
- Fever.
- Night sweating.
- Pruritus.
- There is a painless enlargement of the lymph node.
- Due to the enlargement of lymph nodes, there may be compression and lymphedema.
- Hematological findings are :
- Raised ESR.
- Anemia.
- Eosinophilia.
- Lymphopenia.
- Immunological disturbance leads to depression of T cell function. There are more chances for infection.
- Stage I and II have a survival of 90% for 5 years.
- Stage IV A and IV B have survival 70% for 5 years.
Gross feature
- This disease starts in a single lymph node and then spreads to the adjacent nodes.
- This may start in spleen or thymus.
- Nodular sclerosis may start in the thymus.
- On cut section lymphocytic predominant type has a fish fleshy appearance.
- Mixed cell types may show foci of necrosis.
- Nodular sclerosis type has a fibrous appearance.
| Lymphocytic predominant type | Mixed cell type | Lymphocytic depletion type | Nodular sclerosis |
| 15% | 30% | 15% | 40% |
| More in male <35 years of age | More in male | More in older male | More in females and young adults |
| Mainly mature lymphocytes and variable histiocytes | Lymphocytes are less in number | Increased RS cells and less lymphocytes | Fibrous bands. More collagen tissue |
| Reed Sternberg (RS) cells are rare | RS cells are frequent | Hypocellular | RS cells are Lacunar cell type |
| Little fibrosis | Scanty fibrosis | Diffuse fibrosis | Fibrous bands and collagen |
| No necrosis | Necrosis occasional | Reticular type | Lymphocytic predominant or mixed cell type |
| More lymphocytes | Mimic granuloma | More cellular, pleomorphic cells | Classical RS cells are less common |
| Prognosis excellent | Prognosis intermediate | Prognosis is poor. Aggressive tumor | Prognosis excellent |
Hodgkin’s Lymphoma histology shown in the following table
| Reed Sternberg cells | Lymphocytes | Collagen | Diffuse fibrosis | Eosinophils | Plasma cells | Frequency | 5 years survival | |
| Lymphocytic predominant | rare | ++ to +++++ | 0 | 0 | 0 | 0 | 10% | 90% |
| Mixed cellularity | +++ | ++ to +++ | 0 | ++ | ++ | + | 35 to 60% | 70% |
| Lymphocytic depletion | ||||||||
| Diffuse type | + to +++ | 0 | 0 | ++++ | + | + | 5 to 10% | 20% |
| Reticular type | + to ++++ | + | 0 | + | ++ | + | ||
| Nodular sclerosis | ++ Lacunar cells | + to ++++ | ++ to ++++ | + | + | + | 35 to 60% | 50 to 70% |
Clinical Staging
There is An Arbor staging system given in 1971 by Carbon, P.T. et al
Stage I: There is a single lymph node or extra-nodal organ or site.
Stage II: Two or more lymph nodes region on the same site of diaphragm alone or with the involvement of contagious extra lymphatic organ or tissue (IIE)
Intestine with or without positive lymph nodes.
Stage III: Lymph nodes regions on both sides of the diaphragm which may include spleen (III S) and/or limited contiguous extra-lymphatic organs or site (III E S).
Stage IV: Multiple or disseminated involvement of one or more extra-lymphatic organs or tissue with or without lymphatic involvement.
Stage A and B are on the basis of signs and symptoms like fever, weight loss 10% and night sweating.
The host immune response depends upon the type of disease.
- Good response in H.D lymphocytic predominant and Nodular Sclerosis.
- Intermediate response in Mixed cell type.
- Poor response in H.D lymphocytic depletion type.
There is long term survival due to radiation and chemotherapy.
These patients may develop other malignancies like cancer of lung, stomach, and melanoma.