Erythrocyte Sedimentation Rate (ESR), vs C-Reactive Protein (CRP)
Erythrocyte Sedimentation Rate (ESR)
What is the sample for Erythrocyte Sedimentation Rate (ESR) and C-reactive protein?
- The whole blood sample is taken in EDTA (an anticoagulant). It measures the rate of sedimentation in one hour.
- Or take blood in a 3.8% trisodium citrate solution.
- The sample is stable for 2 hours at 25 °C and 12 hours at 4 °C.
- We require serum for C-reactive protein (CRP) measurement.
What are the indications for Erythrocyte Sedimentation Rate (ESR)?
- It can be done in occult diseases.
- For the diagnosis of acute and chronic infections.
- For collagen vascular diseases.
- In advanced malignancies.
- In tissue necrosis and infarction.
- ESR can be used to monitor disease activity, particularly in autoimmune diseases. It will correlate with disease severity or disease course.
- It is useful for diagnosing and monitoring temporal arteritis and polymyalgia rheumatica.
- It is also used to monitor Hodgkin lymphoma.
What is the Pathophysiology of Erythrocyte Sedimentation Rate (ESR)?
How will you define ESR?
- It is the measure of RBCs settling in diluted plasma over a specified period.
- This is a numeric value in mm over 60 minutes.
What is the principle of ESR?
- This is directly proportional to RBC mass and inversely proportional to plasma viscosity.
- The ESR is the rate at which RBCs settle out of anticoagulated blood in one hour.
- RBCs give rise to more rouleaux formation in abnormal conditions like inflammatory conditions and the necrotic process, resulting in aggregation of the RBCs, which makes them heavier and more likely to fall rapidly so that there are increased RBCs mass, which increases the ESR due to faster settling of RBCs.
- There are two methods:
- Wintrobe method.
- Westergren method.
- This is a nonspecific but not diagnostic test.
- ESR correlates with plasma fibrinogen levels and depends on RBC rouleaux formation.
What factors will affect ESR?
: ESR depends upon")
Erythrocyte Sedimentation Rate (ESR): ESR depends upon
- Inflammatory, neoplastic, infectious, and necrotic diseases increase plasma protein content, primarily fibrinogen, leading to elevated ESR levels.
- ESR is advised in occult diseases.
- Poikilocytosis, therefore, tends to inhibit sedimentation.
- Increased RBC flattening, as in obstructive liver disease, accelerates sedimentation.
- ESR should not be used to screen the asymptomatic patient for disease.
- When ESR is elevated, a careful history and clinical examination will usually diagnose the disease.
- This is a nonspecific test for diagnosing chronic diseases such as tuberculosis and for detecting elevated levels in malignancies and autoimmune diseases.
- Whenever a patient has an elevated ESR, a thorough workup is warranted.
- ESR is raised with aging and anemia.
When patients have an ESR>100 mm/hour, what is the predictive value for serious disease?
- Malignancy, particularly myeloma.
- Infection.
- Collagen vascular disease.
- Rheumatoid Arthritis.
- Renal Disease.
- Sarcoidosis.
When will you see raised ESR?
- Paraproteinemia.
- Multiple myelomas.
- Macroglobulinemia.
- This test is useful for diagnosing and monitoring temporal arteritis and polymyalgia rheumatica.

ESR raised due to factors
What is the effect of Anticoagulants on ESR?
- Sodium citrate and EDTA do not affect the ESR.
- Sodium or potassium oxalate shrinks the RBCs.
- Heparin also causes RBC shrinkage and leads to increased false-positive ESR values.
- EDTA is the anticoagulant of choice.

ESR affecting factors
What are the limitations of ESR?
- First, this is a nonspecific test.
- Sometimes, not elevated in the active disease.
- ESR may be influenced (increased) by other factors like pregnancy, anemia, and a few other diseases.
- Fibrinogen concentration.
- Serum cholesterol level.
- Globulin concentration, specifically gamma globulins.
- Rouleaux formation decreases the surface area.
- Sickle cells fail to form rouleaux, resulting in a low ESR.
What is the Normal ESR?
- Male = 0 to 15 mm/hour.
- Female = 0 to 20 mm/hour.
- >50 years
- Male = 0 to 20 mm/hour.
- Female = 0 to 30 mm/hour.
- Child = up to 10 mm/hour.
- Newborn = 0 to 2 mm/hour.
Another source
- Men = 0 to 5 mm/hour.
- Women = 5 to 15 mm/hour.
- There is a progressive increase in old age.
What are the conditions where ESR is falsely low?
- Sickle cell anemia.
- Spherocytosis.
- Hypofibrinogenemia.
- Polycythemia.
What are the conditions under which the ESR value is reduced?
- High blood glucose (hyperglycemia).
- In the case of raised phospholipids.
- In the case of raised albumin.
- In the case of raised WBCs.
C-Reactive protein:
How will you define C-reactive protein?
- C-reactive protein (CRP) is a substance made by the liver. It rises in the blood during inflammation.
- CRP is a marker of inflammation.
What are the causes of raised CRP?
- Bacterial infection.
- Collagen (inflammatory) diseases like rheumatoid arthritis and vasculitis.
- Tissue injury and trauma.
- Some cancers.
- After surgery.
- Cardiovascular inflammation.
What is the normal CRP?
- Normal CRP = <5 mg/L (<0.8 mg/dL) by nephelometry.
- Normal CRP = 0.02 to 0.800 mg/dL (0.2 to 8.0 mg/L) by immunoturbidimetric assay.
- Mild elevation is seen in viral infection and mild inflammation.
- High CRP level = >50 to 100 mg/L. It is seen in severe infection.
What are the types of CRP?
- Standard CRP = It detects infection and inflammation.
- hs-CRP (high-sensitivity reaction) = It is used for cardiovascular risk.
- Low risk = <1 mg/L.
- Moderate risk = 1 to 3 mg/L.
- High risk = >3 mg/L.
What is the difference between ESR and CRP?
| Clinical parameters | ESR | CRP (C-reactive protein) |
| Normal level |
Men = 0 to 5 Women = 5 to 15 mm/hour |
<1.0 mg/dL |
| Sensitivity | Less sensitive | More sensitive |
| Rise of the CRP/ESR | Slow 24 to 48 hours | Rapid 6 to 8 hours |
| Process of origin | RBC settles in one hour | It is made by the liver |
| Fall after recovery | Slow | Fast |
| Pathophysiology (etiology) | Fibrinogen level goes up in the serum, which causes RBCs to clump together | Dead and dying cells release chemical factors that stimulate the liver to produce CRP |
| Increase in the level of the antibody | No relation to the antibody | CRP Increases before the increase in the antibody level |
| Response to inflammation | Late response |
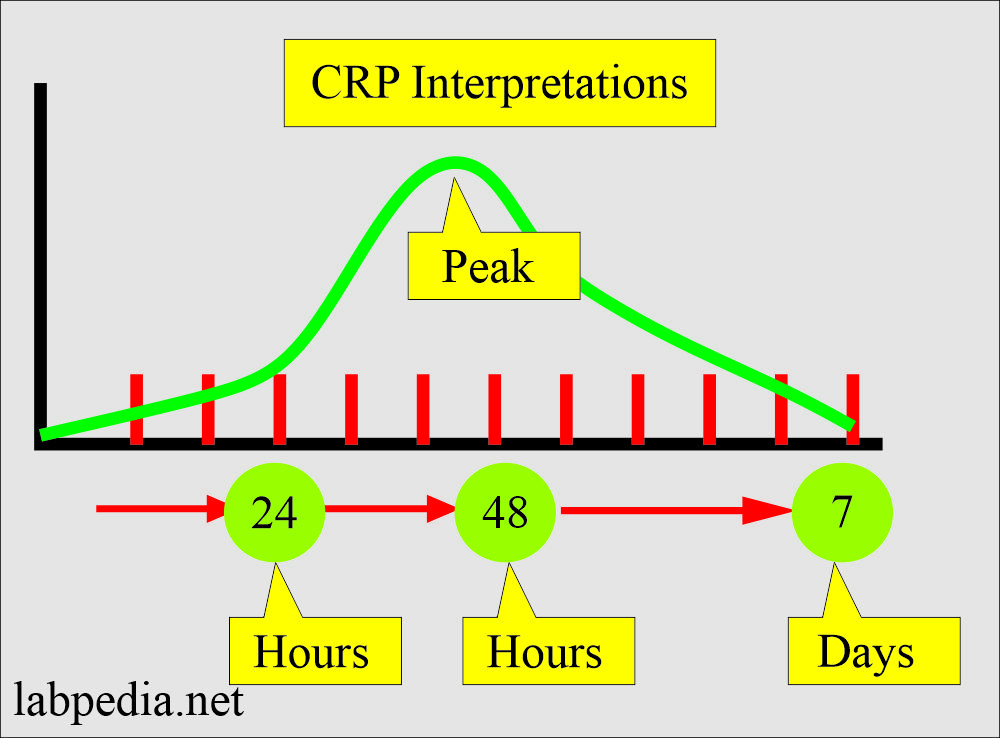 CRP interpretations
|
| After the inflammation | Take more time | Disappears early |
| Acute myocardial infarction | No relation |
|
| Coronary anginal attack | No relation | Normal |
- ESR is a nonspecific test, but it is among the most effective for detecting systemic abnormalities.
- Whenever you find a raised ESR, do not ignore it; perform a thorough workup of the patient. It definitely shows some underlying disease.
Questions and answers:
Question 1: What is the sensitivity of ESR and C-reactive protein?
Question 2: Is there any relation of antibodies to ESR?