Adrenal Gland Hormones Interpretation, (Cortisol and Aldosterone)
Adrenal Gland Hormones
What sample is needed for Adrenal Gland Hormones?
- The serum of the patient is required.
- A urine sample may be used.
- For catecholamines (Epinephrine and Norepinephrine), plasma in heparin or EDTA is needed.
- Transport this plasma on ice, centrifuge at 4 C within 30 minutes, and separate the plasma. Now, freeze till the test is run.
- Urine may be collected for 24 hours. Add 6 M HCl and Refrigerate during collection.
- For Cortisol, Serum is needed. Can use heparinized plasma.
- Urine for 24 hours is collected with the addition of boric acid.
- The serum is stable for 2 days at 2 to 8 °C.
- For aldosterone, a test can be done on plasma (heparin, EDTA, or citrate).
- The serum can also be used.
- The patient must be upright for 2 hours before the sample is taken.
- Urine is collected for 24 hours with boric acid, and during collection, it is refrigerated.
- For Estrogen can be estimated in the serum.
- The serum needs to be frozen immediately after collection.
- A urine 24-hour sample is collected with the addition of boric acid.
What are the precautions before performing the Adrenal gland tests?
- A fasting sample is needed.
- Avoid exercise or physical activity.
- Reduce stress before performing this test.
- Avoid herbal medicines and any medication that interferes with the test.
- Avoid a nuclear scan before this test.
- The aldosterone AM sample is higher than PM.
- Cortisol’s highest level is 8 AM and >50% less at 8 PM.
- Transport the plasma on ice to the lab.
- Centrifuge at 4 °C.
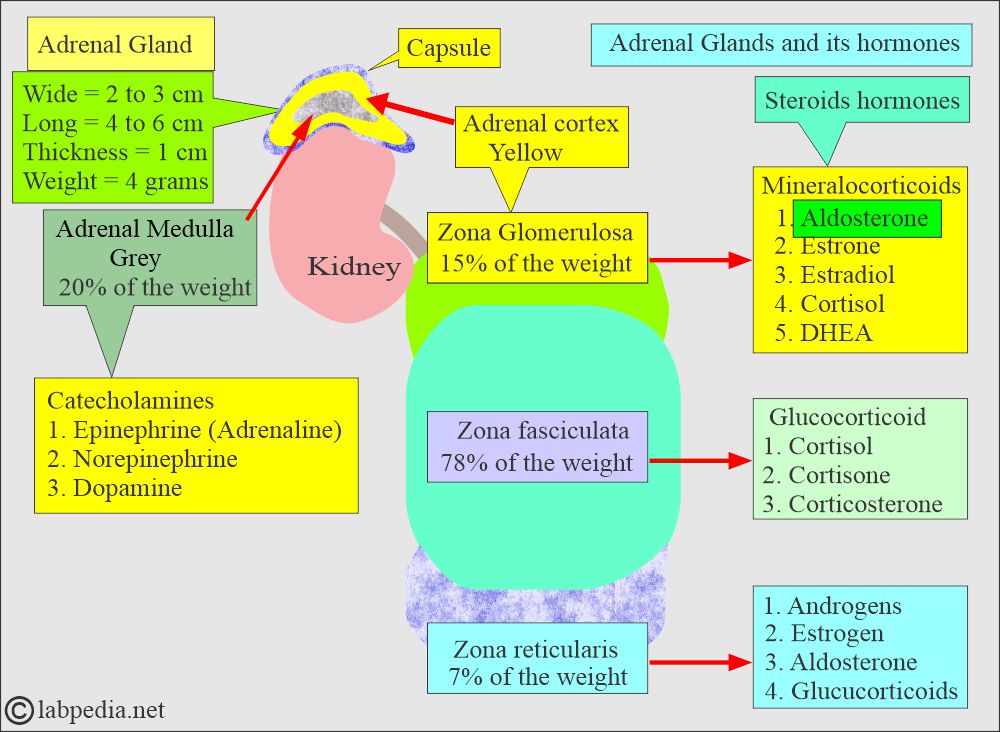
What is the anatomy of adrenal glands?
- Adrenal glands consist of the following:
- The adrenal medulla is grey.
- The adrenal cortex is yellow.
- The adrenal cortex is derived from the mesoderm.
- These hormones maintain the homeostasis of the body.
- The adrenal medulla is derived from the ectoderm.
- Adrenal gland measure:
- Wide = 2 to 3 cm.
- Length = 4 to 6 cm.
- Thickness = 1 cm.
- Weight approximately = 4 grams (regardless of age and sex).
What are the adrenal cortex hormones?

Adrenal gland hormones
What is the fate of Steroid hormones?
- These are synthesized from the cholesterol in the adrenal glands and gonads.

Adrenal cortex hormone formation
- The nature and quantity of the steroid hormone produced by the adrenal glands and gonads differ.
- The ovaries and testes contain enzymes synthesizing male and female sex hormones.
- Steroid hormones circulate in the blood in free and bound forms.
- In plasma, these are bound to the carrier protein or albumin.
- Steroid hormones conjugate to glucuronide or sulfate and are excreted by the kidneys or gastrointestinal tract.
- 90% to 96% of steroids have a high affinity for the carrier protein globulin.
- 60% to 70% of the circulating steroids are bound to albumin, which has a low affinity for carrier protein.
- Androgens produced by the theca cells of the ovary are converted to estrogen.

Androgens to estrogen conversion
What is the origin of mineralocorticoid?
- The primary example of mineralocorticoid is aldosterone.
- It is produced in the zona glomerulosa of the adrenal cortex.
- Aldosterone regulates sodium and potassium.
- Other examples of endogenous mineralocorticoids are progesterone and deoxycorticosterone.
Discuss the Aldosterone?
- It is the major Mineralocorticoid produced by the adrenal cortex, 200 µg/day.
- It promotes renal K+ excretion and increases water retention by increasing renal Na+ retention.
- It increases the plasma concentration of the Na+ by increasing the Na+ absorption in the renal tubules.
- Aldosterone is present in a very minute amount in the plasma, making it difficult to measure accurately.
- If someone stands for a long time, his plasma aldosterone level will be between 5 and 20 ng/dL.
- If the person is lying for several hours, the aldosterone level will fall and maybe 10% to 40% less than in the upright position.
- What is the metabolism of Aldosterone?
- The liver converts aldosterone into glucuronide and tetrahydro-glucuronide; this will be excreted in the urine.
- Kidneys also inactivate aldosterone by changing it into water-soluble glucuronide.
- How would you describe Hyperaldosteronism?
- It is usually due to an adrenal tumor that has S/S of:
- Increased serum Na+.
- Decreased K+.
- Hypertension.
- Plasma aldosterone level is increased.
- Urine excretion of aldosterone is also increased.

Role of the aldosterone
What are the causes of Primary aldosteronism?
- Adrenal tumor, usually adenoma of the adrenal cortex.
- Bilateral nodular hyperplasia.
What are the causes of Secondary aldosteronism?
- Low serum Na+ level.
- ACTH
- High serum K+ level.
How will you differentiate Primary aldosteronism from secondary aldosteronism.?
| Lab test | Primary aldosteronism due to | Secondary aldosteronism | ||
| Hyperplasia | Adenoma | Edema (CCF and Cirrhosis) | Accelerated Hypertension | |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What is the differential diagnosis of adrenal adenoma, carcinoma, and idiopathic hyperplasia?
| Lab test | Adenoma | Adrenal carcinoma | Idiopathic hyperplasia |
| Plasma renin activity | Suppressed/ very low | Suppressed/ very low | Not markedly suppressed |
| Plasma /urine aldosterone | Increased | Markedly increased | Usually mild increase |
| Hypokalemia | Increased | More marked increase | Not markedly increased |
| Aldosterone response to posture | Decreased or not increased (70% to 80%) | Often unchanged /or random increase | Increased in all cases |
| Excess hormone production |
|
|
|
Discuss the Glucocorticoids?
- Cortisol is the most potent glucocorticoid.
- It is like cortisol, which is gluconeogenic.
- Cortisol is produced at 25 mg/day by the adrenal cortex.
- It regulates intermediary carbohydrate metabolism.
- What are the functions of glucocorticoids?
- It has a metabolic function.
- It has an inflammatory function.
- This is also anti-inflammatory.
- It has a growth-suppressing effect.
- It influences the level of awareness and sleep patterns.
- Glucocorticoids have a direct effect on glucose levels, and it increases the glucose level.
- Glucocorticoids’ main function is in Carbohydrate metabolism.
- There is gluconeogenesis in the liver.
- There is a decrease in glucose levels in the muscle, adipose tissue, and lymphatic tissue.
- In extrahepatic tissue, Glucocorticoids antagonize insulin.
Discuss the Cortisol?
- Cortisol is the most potent naturally occurring glucocorticoid.
- The daily secretion of cortisol is 25 mg/day.
- But the plasma shows a level of 6 to 25 µg/dL.
- Cortisol is formed from the cholesterol in the zona fasciculata and zona reticularis of the adrenal cortex.
- When cortisol is released into the circulation, it binds with corticosteroid-binding globulin and is transported as such.
- What are the metabolic functions of cortisol?
- Cortisol is metabolized and conjugated in the liver into several inactive forms.
- >90% of cortisol and its metabolite cortisone is conjugated with glucuronic acid and excreted in the urine as a conjugate.
- <2% of cortisol, which is not metabolized, is excreted in the urine as free cortisol.
- Cortisol and its oxidation product, cortisone, are inactivated in the liver by two separate processes:
- The reduction process is hydrogenation to tetrahydro derivatives.
- These products are conjugated with glucuronic acid and excreted in the urine.
- 30% to 50% of these appear as glucuronide conjugates of tetrahydro-derivates of cortisol and cortisone.
- All these compounds contain a dihydroxyacetone group in the side chain, known as 17-hydroxycorticosteroid (17-OHCS).
- The RIA kits can chemically estimate 17-hydroxycorticosteroid (17-OHCS). In the past, the Porter-Silber reaction was used, but it is now obsolete.
- Determining plasma cortisol is useful in diagnosing both hypo- and hyperconditions adrenocortical diseases.
- Not >1% of the total cortisol synthesized in the body daily is excreted as such in the urine.
- What are the functions of the cortisol?
- Cortisol acts on the target cells by penetration and transport to the cell nucleus.
- It will bind the DNA and alter the transcription of RNA.
- Cortisol alters the various metabolic processes.
- It accelerates the enzymatic breakdown of muscle proteins and the conversion of their amino acids into glucose.
- Fat is metabolized for the provision of energy.
- Cortisol acts antagonistic to insulin action by inhibiting glucose uptake by the muscles.
- It decreases the cellular reaction to the inflammatory agents.
- It decreases antibody formation, leading to poor immune response.
- This is the main hormone of the adrenal cortex that maintains life and protects the body from stress.
- Hypothalamus hormone CRH travels through the portal circulation to stimulate the production of ACTH, β-lipoprotein, γ-lipoprotein, endorphins, and enkephalins by the anterior pituitary.
- Cortisol secretions follow ACTH stimulation of the adrenal cortex, and ACTH is the main regulator of cortisol secretion and adrenocortical growth.
- How is Cortisol transported in the plasma?
- 85% is transported by corticosteroid-binding globulin (CBG called transcortin).
- 10% bound to albumin.
- 5% is in free form (not bound to proteins).
- The cortisol follows the ACTH pattern; it is high early in the morning and lowest at midnight.

Cortisol circadian rhythm
- Cortisol inhibits the secretion of ACTH from the pituitary gland and also inhibits CRH from the hypothalamus.

Cortisol inhibitory function
What are the Adrenal androgens?
- It is like such as dehydroepiandrosterone (DHEA) and androstenedione. These are also called sex hormones.
- The adrenal androgens include:
- DHEA is the principal androgen, secreted at 20 mg/day.
- Testosterone (converted to estradiol).
- DHEA is converted to Androstenedione, which in turn is converted to estrone.
The adrenal medulla
What are the hormones of the adrenal medulla?
- It is a neuroendocrine gland that secretes:
- Epinephrine.
- Norepinephrine.
- Both act on the sympathetic nervous system.
- These hormones regulate the acute response of the body to external stimuli.

Adrenal gland hormones
Adrenal gland’s hormone and their action
Discuss the ACTH hormone?
- ACTH (Adrenocorticotropin hormone) from the pituitary gland stimulates the adrenal cortex.
- After the stimulation of the adrenal cortex by the ACTH, the process of steroidogenesis starts with cholesterol.
- The pituitary gland (ACTH) is stimulated by the Hypothalamic hormone (Corticotropin-releasing factor (CRH).

ACTH and the Role of CRH
- Serum ACTH level has a diurnal variation:
- The peak level is at 7 AM at about 200 pg/ml.
- ACTH level declines and the lowest level is around 100 pg/ml at midnight.
- What are the factors for ACTH secretion?
- High circulating levels of cortisol suppress ACTH and CRH.
- At the same time, the low level of cortisol stimulates their secretion.
- There is diurnal variation in the secretion of ACTH and cortisol levels. There is a sleep-wake pattern.
- ACTH peak is 3 to 5 hours after sleep begins and declines throughout the day. Cortisol follows the same pattern.
- Stress increases ACTH secretion, which leads to increased cortisol levels.
- The peak level is from 8.00 to 9.00 AM. The highest level is early morning, and the lowest is midnight.
What are the normal levels of adrenal gland hormone?
- Epinephrine = <50 pg/mL
- Urine epinephrine = 0 to 20 µg/ day
- Norepinephrine = 110 to 410 pg/mL
- Urine norepinephrine = 15 to 80 µg/ day
- Dopamine = <87 pg/mL
- Urine dopamine = 65 to 400 µg/ day
- Cortisol Total
- Cord blood = 5 to 17 µg/dL
- Infants = 2 to 11 µg/dL
- Child 1 to 16 years at 8 am = 3 to 21 µg/dL
- adult 8 am = 5 to 23 µg/dL
- 4 pm = 3 to 16 µg/dL
- Urine cortisol (free) =
- Adult = 20 to 90 µg/ day or (<100 µg/day)
- Child = 2 to 27 µg/day
- Aldosterone
- Cord blood = 40 to 200 ng/dL
- Full-term infant 3 days = 7 to 184 ng/dL
- Infants 1 to 12 months = 5 to 90 ng/dL
- Children 1 to 2 years = 7 to 54 ng/dL
- Children 2 to 10 years =
- Supine position = 3 to 35 ng/dL
- Upright position = 4 to 48 ng/dL
- Adult
- Supine position = 3 to 16 ng/dL
- Upright position = 7 to 30 ng/dL
- Estrogen Total
- Male = 20 to 80 pg/mL.
- Female
- Luteal phase = 160 to 400 pg/mL.
- Follicular phase = 60 to 200 pg/mL.
- Postmenopausal = <130 pg/mL
What is the outcome of Adrenal Hyperfunction?
- Excess of Cortisol causes Cushing’s syndrome.
- Excess of Aldosterone causes Hyperaldosteronism.
- Excess of Androgens causes Virilizing syndrome.
What are the findings of Primary Hyperadrenalism?
- The cortisol level is raised.
- ACTH level decreases.
What are the lab findings on primary adrenal insufficiency (Addison’s disease)?
- This is due to the diseases of the gland.
- The cortisol level is decreased.
- Serum sodium is low.
- The glucose level is decreased.
- ACTH level is raised.
- Potassium, calcium, and blood urea are raised.
What are the lab findings of Secondary Hypoadrenalism (secondary or tertiary Adrenal insufficiency)?
- This is due to external factors that lead to the under-activity of the glands.
- Cortisol level is decreased.
- ACTH level is low.
What are the lab findings of Cushing’s syndrome?
- There is no diurnal variation of ACTH, and it is absent.
- There is an elevated level of Cortisol, Glucose, and Sodium.
- There is a decreased Potassium level.
What are the lab findings of Adult adrenogenital syndrome?
- There is an elevated level of:
- DHEA
- Urine 17- ketosteroids
- ACTH
- There is a decreased level of:
- Cortisol
What are the lab findings of Congenital Adrenal Hyperplasia:
- There is an elevated level of:
- ACTH
- Androgens level
- Decreased level of:
- Cortisol
- Aldosterone
What are the lab findings of Primary Hyperaldosteronism (Conn’s syndrome)?
- There is an elevated level of:
- Aldosterone urine and blood
- Serum sodium
- There is a decreased level of:
- Potassium.
- Renin.
- No response to the aldosterone suppression test.
Questions and answers:
Question 1: What are the lab findings in Cushing's syndrome?
There is no diurnal variation of ACTH, there is raised level of cortisol, glucose, and sodium. There is a decreased level of potassium.
Question 2: What are the lab findings of Addison's diseases?
Cortisol level is decreased. Serum sodium is low, and glucose is low. ACTH level is raised. Blood urea, calcium, and potassium are raised.
Informative content.. thx
Thanks.
Useful in sexual development & sexual disorder
Thank you for your useful information
Thanks.