ACTH (Adrenocorticotropic Hormone), Cushing’s Syndrome
ACTH (Adrenocorticotropic Hormone)
What sample is needed for Adrenocorticotropic Hormone (ACTH)?
- The Patient’s plasma is needed.
- Place blood immediately in ice water and freeze plasma for 15 min.
- The sample should be collected in a prechilled plastic test tube with EDTA or heparin.
- Transfer the sample immediately to the lab on ice.
- For the diagnosis of Cushing’s syndrome, the sample should be taken between 6 to 11 pm.
- Centrifuge the sample at 4 °C and store it at -20 °C immediately within 15 minutes of collection.
What are the precautions for Adrenocorticotropic Hormone (ACTH)?
- A stressful collection of blood will raise the level.
- Stress, mental or physical, and obesity can increase the value.
- Ask the patient to relax and reduce environmental stress.
- Avoid physical activity 10 to 12 hours before taking the sample.
- Physical activity increases the value.
- Ask the patient not to eat or drink after midnight on the night before samples are taken.
- Stop medication like corticosteroids 48 hours before this test.
- Collect the sample in a chilled plastic vial with EDTA or Heparin.
- ACTH is very labile and requires antiprotease in the collecting vial.
- The ACTH level is not measured in the routine because it degrades in the plasma.
- Put the patient on a low-carbohydrate diet.
- Oral contraceptives can decrease their value.
- Glucocorticoids and estrogen decrease the value.
- Blood glucose interferes with the accurate value.
- A radioactive scan within one week of the test will interfere with accurate results.
What are the Indications for Adrenocorticotropic Hormone (ACTH)?
- This hormone is estimated in various conditions like Adrenal insufficiency, Cushing’s syndrome, and Acromegaly.
- For the diagnosis of Addison’s disease (level is>1000 pg /ml).
- Its level decreases in Secondary Adrenocortical Insufficiency, Adrenal carcinoma, and adenoma.
- This is the test of the anterior pituitary gland.
How will you define adrenocorticotropic hormone (ACTH)?
- Adrenocorticotropic hormone (ACTH) is a peptide hormone produced and secreted by the anterior pituitary gland.
- Its primary functions are:
- Stimulate adrenal glands to produce and secrete cortisol.
- Cortisol is a glucocorticoid hormone that plays an important role in metabolism, immune response, and stress.
- The anterior pituitary gland is considered the master gland due to the many hormones secreted by this gland.
- The hormones secreted are TSH (Thyrotropin), ACTH, and reproductive hormones like FSH, LH, and many others.
What are the anterior pituitary lobe hormones?
| Hormone | Chemical nature | Target organ | Main function |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What are the main functions of the Adrenocorticotropic Hormones (ACTH):
- These hormones maintain a constant internal environment in the body fluid, leading to homeostasis.
- It will regulate the growth and development of the body as a whole.
- It will regulate energy production and stabilize the metabolic rate (system).
- It will help the body to adjust to a stressful or emergency state.
- It will promote sexual maturation, maintain the sexual rhythm, and help the reproductive process.
- Summary of the ACTH hormone functions:
- Stimulate cortisol production.
- It regulates the body’s stress response.
- It maintains blood pressure.
- It maintains body metabolism.
What is the ACTH hormone solubility?
- Hormones that are soluble in plasma are from:
- Hypothalamus.
- Anterior and posterior pituitary.
- Pancreas.
- Parathyroid.
- Hormones that are poorly soluble in plasma and will need plasma proteins as a carrier are from:
- Adrenal cortex.
- Gonads.
- Thyroid.
- Pituitary glands consist of:
- Anterior lobe (adenohypophysis).
- Posterior lobe (neurohypophysis).
Adrenocorticotropin hormone (ACTH):
What is the significance of the Adrenocorticotropin hormone (ACTH)?
- The adrenal gland is present at the upper pole of the kidneys.
- It consists of the adrenal cortex and adrenal medulla.
: Adrenal gland location")
ACTH (Adrenocorticotropic hormone): Adrenal gland location
- ACTH is a tropic hormone. It is a long-chain polypeptide that binds to adrenal cortex cells and influences their activities.
- ACTH is a 39 amino acid peptide hormone secreted by the anterior pituitary gland.
- The anterior pituitary hormones are produced in a pulsatile pattern.
- Basal level = close to 5 pg/mL.
- Highest level = 6 to 8 A.M.
- Lowest level = 6 to 11 P.M.
- The plasma level of ACTH does not exceed 50 pg/mL.
- Anterior pituitary hormones are either tropic, which means their action is specific for another endocrine gland, or are direct effectors because they act directly on the peripheral tissue.
 formation")
Adrenocorticotropic (ACTH) formation
- Corticotropin-releasing hormone (CRH) is made and released from the hypothalamus, giving rise to ACTH release from the pituitary glands.
- CRH stimulates ACTH production in the anterior pituitary gland.
- Now, ACTH sends signals to the adrenal gland (cortex), which secretes steroids (cortisol, androgen, and aldosterone).
- The rising cortisol level is a negative feedback mechanism that stops CRH and ACTH production.
: ACTH and role of CRH")
ACTH (Adrenocorticotropic hormone): ACTH and the Role of CRH
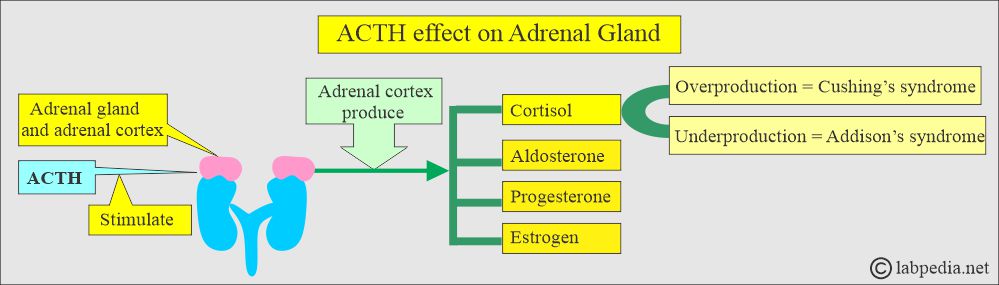
ACTH effect on the adrenal gland
What are the peaks of adrenocorticotropic hormone (ACTH) secretion?
- ACTH is released in a burst, so its level can vary from minute to minute.
- Highest between 6 to 8 AM.
- The lowest level is between 9 to 10 (6 to 11) PM.
- During sleep, it is at the normal level.

ACTH level for 24 hours
- Pregnancy, menstrual cycle, and stress increase secretion.
- ACTH is released in response to many stresses.
- ACTH is advised for investigating disorders of the hypothalamic, pituitary, and renal systems.
- ACTH is secreted by the anterior pituitary gland, which signals the adrenal gland to produce steroids (androgens, cortisol, and aldosterone). These are needed for the body’s normal functioning.
- With adrenal insufficiency, the pituitary gland releases proopiomelanocortin, increasing ACTH.
- ACTH is unstable in the blood. Most commercial RIA kits are insensitive and nonspecific when measuring ACTH.
What is the normal Adrenocorticotropic Hormone (ACTH)?
Source 2
- 6 to 8 a.m = <80 pg / mL or <18 pmol /L (SI units).
- 6 to 11 p.m = <50 pg /mL or <11 pmol /L (SI units).
- or less than 120 pg/ml
Another reference gives the following values:
- 8 AM ( unrestricted activity) = <120 pg/mL
- 4 to 8 PM <85 pg/mL
- Cord blood = 50 to 570 pg/mL
- Newborn = 10 to 185 pg/mL
Another reference gives the following values:
Adults, Adolescents, children, and elders
- 8 A.M. fasting = 15 to 100 pg/mL (10 to 80 ng/L)
- 4 P.M. nonfasting = 10 to 50 pg/mL (10 to 50 ng/L)
- Newborn = 10 to 185 pg/mL
Cushing’s Syndrome
How will you define Cushing’s syndrome?
- Cushing’s syndrome is named after the name of Dr. Harvey Cushing, who was the surgeon.
- Cushing’s syndrome is a hormonal imbalance caused by prolonged exposure to increased cortisol levels.
- Cushing’s syndrome may be caused by:
- Endogenous overproduction of cortisol by the adrenal glands.
- Exogenous when there is overuse of corticosteroids.
What are the causes of Cushing’s Syndrome?
- As a result of treatment with corticosteroids, this is the nonadrenal cause.
- Secondary to a benign hormone-secreting pituitary adenoma. These are ACTH-secreting adenomas (68%).
- Cortisol production from the adrenal tumors or nodules (17%).
- Excess ACTH ectopic production (15%). Mostly, there are malignant tumors.
- Chronic alcoholism, stress, and obesity.
What is the clinical presentation of Cushing’s syndrome?
- This may be a form of Hyperadrenalism or Hypercortisolism with common clinical presentations.
- These patients have similarities like diabetes mellitus type 1 (insulin resistance).
- There are 4 times increased mortality even after successful treatment.
- Patients have cardiovascular diseases. There is left ventricular hypertrophy.
- There are changes in the ECG and nocturnal hypotension.
- Blood pressure changes were seen in 85% to 90%.
- Central obesity is seen in 90%.
- Glucose intolerance is seen in 80%.
- Hirsutism is seen in 65%.
- There are abnormal menses by 60%.
- There may be muscle weakness in 60%.
- Untreated cases have a 50% mortality for 5 years.

Cushing’s syndrome clinical presentation

Cushing’s syndrome appearance
How will you diagnose Cushing’s syndrome?
- The abnormal Overnight Dexamethasone suppression test and 24-hour urinary cortisol test are diagnostic of Cushing’s Syndrome.
- The free urinary cortisol level (24-hour sample) is the most sensitive, 95% to 100%, and specificity is 98%.
- Random plasma cortisol level is of little value for diagnosing Cushing’s syndrome.
- There is a loss of diurnal rhythm because late-night values remain high.
- The ideal time for collecting ACTH and cortisol is between 11.00 p.m. and 12.00 a.m.
- A single midnight serum sample concentration >7.5 µg/dL is diagnostic of Cushing’s syndrome with a sensitivity of 90% to 96% and specificity of 100%.
- The salivary cortisol level at 11.00 p.m., when combined with the 8.00 a.m. salivary cortisol concentration after the 1 mg overnight dexamethasone suppression test, had a sensitivity and specificity of 100%.
- Radiological work-up:
- Adrenal gland CT distinguishes hyperplasia vs. tumor.
- Adrenal MRI distinguishes the carcinoma.
- Pituitary CT diagnoses 85% of microadenoma.
- CT scan finds ectopic ACTH sources like bronchial adenoma, medullary thyroid carcinoma, and squamous cell carcinoma.
- The ACTH level is high when Cushing’s syndrome is due to a Pituitary or ectopic source.
- When the source is the Adrenal gland, the ACTH is low.
How will you differentiate between Cushing’s syndrome and Addison’s disease?
| Disease | ACTH value | Cortisol value |
|---|---|---|
| Cushing’s syndrome |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Addison disease | ||
|
|
|
|
|
|
|
|
|
What are the causes of increased ACTH levels?
- Addison disease (primary adrenal insufficiency).
- Ectopic ACTH syndrome.
- Cushing’s syndrome. This is dependent upon adrenal hyperplasia due to the pituitary gland.
- Stress.
What are the causes of decreased ACTH levels?
- Hypopituitarism.
- Secondary adrenal insufficiency is due to pituitary insufficiency.
- Adrenal adenoma or cancer.
- Exogenous steroid administration.
What is the value of ACTH for the Layman?
- This test is advised if the patient has diabetes mellitus, reduced glucose tolerance, and muscle wasting to rule out Cushing syndrome.
- If there are truncal obesity and thin extremity.
- In case of abnormal lipid metabolism.
Questions and answers:
Question 1: What is the basic mechanism of Cushing's syndrome?
Question 2: What is the source of ACTH?