White blood cells:- Part 1 – White Blood Cells (WBC) Development, Functions, and Interpretations
White Blood Cells (WBC)
What sample is needed for White Blood Cells?
- This is done on EDTA blood.
- The whole blood in EDTA is stable for 24 hours at 23° C and 48 hours at 4 °C.
- Don’t use heparin.
What are the indications for White Blood Cells?
- This is the routine test in CBC.
- TLC differentiates acute and chronic infections.
- TLC diagnoses leukemias.
- TLC is done as a follow-up test in patients on chemotherapy.
- This will help a patient with an allergy.
What are the Precautions for White Blood Cells?
- Physical activity and stress may cause an increase in WBCs and differential values.
- Pregnancy in the final months may cause an increase in WBC count.
- Patients with splenectomy have a persistent mild increase in the WBC count.
- Drugs that may increase the WBC county are:
- Aspirin.
- Allopurinol.
- Steroids.
- Quinine.
- Epinephrine.
- Adrenaline.
- Chloroform.
- Heparin.
- Drugs that will decrease the WBC count:
- Antibiotics.
- Anticonvulsant.
- Antimetabolites.
- Antithyroid drugs.
- Diuretics.
- Sulfonamides.
- Barbiturates.
- Chemotherapy.
How will you discuss the pathophysiology of White Blood Cells?
How will you define hematopoiesis?
- This is the dynamic process of blood cell production and development of the various blood cells.
- All these cells develop from the totipotent stem cells.
- The constant turnover of the blood cells characterizes this hematopoiesis.
- The normal hematopoietic system maintains a cell population of erythrocytes, white blood cells, and platelets through a complex network of tissues, stem cells, organs, and regulatory factors.
What are the functions of the hematopoietic components (cells)?
- It transports oxygen and excretes CO2 through RBCs.
- It fights infection by the WBCs.
- It performs the immune function (cellular and humoral immunity) through the lymphocytes.
- It maintains (hemostasis) the bleeding and the clotting process through the platelets.
How will you discuss the development of myeloid (myelopoiesis) /erythroid (erythropoiesis) cells?
- In the first few weeks of gestation, the yolk sac (mesoderm) is the main site of hematopoiesis. The first stem cells for hemopoiesis are observed in the dorsal aorta, in a region called the aorta-gonads-mesonephros.
- These common precursors of endothelial and hematopoietic cells will seed the bone marrow, liver, and spleen from 6 weeks until 7 months of fetal life.
- The liver and spleen are the major hematopoietic organs and blood cells are produced until around two weeks after birth.
- Marrow is the only source of new blood cells during childhood and adulthood.
- In adult life, the marrow consists of approximately 50% of the fats.
- After 4 years of age, fat cells start appearing in the long bones.
- 18 to 20 years, hematopoiesis is only found in the sternum, ribs, pelvis, vertebra, and skull.
- After 40 years, the sternum, ribs, vertebra, and pelvis comprise 50% fat and 50% hematopoietic tissue.

Hematopoiesis in fetus
How will you discuss the bone marrow activity?
- Bone marrow hematopoietic activity is divided into two pools:
- Stem cells pool.
- Bone marrow pool.
- Eventually, these cells mature and are released into the peripheral blood.
")
Hematopoiesis (Bone marrow)
Hematopoiesis:
- Hematopoiesis starts from the pluripotential stem cells.
- Hematopoietic stem cells are rare; these are 1 in every 20 million nucleated cells.
- There is self-renewal of the stem cells. So, the bone marrow cellularity remains constant in a normal, healthy person.
- There is an amplification of the stem cells, and one stem cell can produce about 106 mature blood cells after 20 subdivisions.
- There are various types of stem cells that develop from the totipotent cells.
- Totipotent cells:
- These are called embryonic stem cells and gave rise to:
- Hematopoietic stem cells give rise to myeloid and lymphoid cells.
- Epithelial stem cells give rise to organs like the liver, etc.
- Mesenchymal stem cells give rise to muscles, tendons, and cartilage.
- Neural stem cells give rise to neural tissue.

Differentiation of stem cell
- These parent stem cells have CD34+ and CD38– and have the appearance of small, medium-sized lymphocytes.
- These stem cells give rise to committed stem cells, which occur under the influence of CFU (colony-forming unit).
- This whole process is shown in the following diagram.

Maturation of all bone marrow hematopoietic cells
How will you divide White blood cells?
- Granulocytic series:
- These cells contain granules in their cytoplasm. Because of a multilobate nucleus, these are also called polymorphonuclear leukocytes (Polys or PMN). These are of the following types:
- Neutrophils.
- Eosinophils.
- Basophils.
- Agranulocytic series:
- These are without any granules in their cytoplasm. These are also called mononuclear cells. These are :
- Lymphocytes.
- Monocytes.
- Platelets.

White blood cell maturation
Can you divide White blood cells in another way?
- Phagocytic cells:
- Neutrophils (polymorphonuclear leucocytes, PMN).
- Eosinophils.
- Basophils.
- Monocytes.
- Immunocytic cells:
- Lymphocytes.
- Lymphocytes precursors.
- The Polys and lymphocytes comprise 75% to 90% of the total WBC count.
How will you discuss Polymorphonuclear leukocytes (PMN)?
- The neutrophils develop from the myeloblast, transforming into promyelocytes, myelocytes, metamyelocytes, band forms, and neutrophils delivered into the peripheral blood.

WBC maturation cycle
How will you discuss the development of the neutrophils?
- These are also called segmented neutrophils or polymorphonuclear neutrophils (PMN).
- The neutrophils are of two types:
- Segmented neutrophils are found in the peripheral blood.
- The cytoplasm stains light blue and has a fine lattice-like structure.
- Granules vary in number and stain, which will be red to blue.
- These cells have large, round, or oval nuclei with coarse chromatin.
- Nucleoli are conspicuous and stain light blue.
- Tissue neutrophils have ample cytoplasm, irregular, blunt pseudopodia that are often multi-pointed, and may have hazy cytoplasmic streamers.
- These cells are not phagocytic and seldom have cytoplasmic vacuoles.
What are the cytokines involved in these phagocytic cells?
| Growth factors/cytokines | Target cells |
|
|
|
|
|
The precursor of:
|
|
|
|
|
What is the life span of white blood cells?
- The leukocytes’ total lifespan is 13 to 20 days, and they are produced in 7 to 14 days from the myeloblastic cells.
- Their life in the peripheral blood is just 7 to 10 hours, and they migrate to the tissue and are replenished by other cells released from the marrow.
- The polys have a dense nucleus consisting of 2 to 5 lobes and pale cytoplasm, with many fine pink-blue (azurophilic granules) or grey-blue granules present in the lysosomes.
How would you divide White blood cell granules?
- Primary granules appear at the promyelocytic stage.
- These contain myeloperoxidase, acid phosphatase, and other hydrolases.
- Secondary (specific) granules appear at the myelocytic stage and predominate in the mature neutrophils.
- These granules contain collagenase, lactoferrin, and lysozyme.
What is the role of the lysosomal enzyme in destroying the bacteria by the neutrophils?
- Bacteria are phagocytosed into cells and fuse with the primary lysosomes to form a phagosome.
- Primary granules attack the bacteria.
- Secondary granules fuse with the phagosomes, and secondary enzymes attack the bacteria.
- Activated oxygen generated by glucose metabolism will kill the bacteria.
- Undigested, killed residual bacterial products are excreted by exocytosis.

White blood cells’ Role in Bacterial Infection
What are the functions of Poly (PMN)?
- The poly (PMN) gives immunity by fighting against infections and reacting against foreign bodies by various methods:
- Phagocytosis is the killing and digestion of bacteria.
- Eosinophils are involved in allergic reactions.
- Eosinophils have a role in parasitic infestation.
- Basophils of the peripheral blood are also rich in histamine granules; they play a role in allergic reactions.
- Monocytic cells have the property of phagocytosis. They can kill bacteria and remove debris.
- Monocytes produced interferon.
- They have a longer life than neutrophils.
How will you summarize the difference between various granulocytic series (neutrophils) cell types?
| Characteristics | Myeloblast | Promyelocyte | Myelocyte | Metamyelocyte | Band form | Neutrophil |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Monocytes:
How will you define monocytes?
- Monocytes develop from the monoblast in the bone marrow.
- These macrophagic cells measure 25 to 80 µm with round or reniform nuclei and contain one or two nucleoli.
- There is clumped chromatin, abundant cytoplasm with vacuoles, and numerous azurophilic granules.
- These monocytes enter the circulation for a short time, then migrate to the tissue and transform into macrophagic cells.
- Monocytes are also called histiocytes, meaning histio = tissue and cyte= = cells.

Monocytes in the peripheral blood smear
What are the various forms of monocytes?
- When these monocytes are mature, they become too large to pass readily through the capillaries, so these settle in the tissue and convert into tissue macrophages in many organs like:
- In the lungs, they are called pulmonary alveolar macrophages.
- In the peritoneum are called peritoneal macrophages.
- In the spleen are called splenic macrophages.
- In the liver are called Kupffer’s cells.
- In the connective tissue are called tissue macrophages.
- These are also phagocytic cells.
- Monocytes don’t enter the circulation but can return to circulation in case of inflammation.
- What are the functions of monocytes?
- Their function as phagocytosis is similar to neutrophils.
- Monocytes can produce more rapidly than neutrophils and spend longer than neutrophils.
Basophils:
How will you define basophils?
- These cells all pass through the same stages as the neutrophils.
- These are also called mast cells when present in the tissue.
- The cells have large basophilic granules.
- The maturation of the basophils in the bone marrow takes more than 7 days.
- Basophils circulate in the peripheral blood for a few hours, then migrate to the tissue, skin, mucosa, and serosal surfaces.

Morphology of the Basophil
Eosinophils:
How will you define eosinophils?
- Eosinophils develop 3 to 6 days in the bone marrow before appearing in the peripheral blood.
- These are stored in the bone marrow and released to the peripheral blood circulation when needed.
- The mean time in the circulation is about 8 hours.
- Eosinophils migrate from blood to bronchial mucosa, skin, GI tract, and vagina in about 12 days.
- Eosinophils can migrate back to blood and bone marrow.
- Eosinophils are motile and can migrate between the endothelial cells into tissue or areas of inflammation.

Eosinophils structure
What are the granules of the eosinophils?
- It contains hydrolytic enzymes like:
- Peroxidase.
- Acid phosphatase.
- Aryl sulfatase.
- β-glucuronidase.
- Phospholipase.
- Cathepsin.
- Ribonuclease.
- But eosinophils lack the enzymes like:
- Alkaline phosphatase.
- Lysosomes.
- Cationic proteins.
- There are tissue eosinophils, and these have prominent nucleoli.
Immunocytes:
How will you define lymphocytes?
Lymphocytes are of two types:
- B – lymphocytes give rise to antibody-dependent immunity.
- T – lymphocytes give cell-mediated immunity; their subtypes are:
- T – cytotoxic cell. (T – killer).
- T – suppressor cell.
- T – helper cell.
- T cells’ primary function is to fight chronic bacterial and viral infections.
What is the normal Total leucocyte count?
Source 2
- Adult /child = 5000 to 10,000 /cmm
- Child ≤2 years = 6200 to 17000 /cmm.
- Newborn = 9000 to 30,000 /cmm
Other sources
- Adult and child = 5000 to 10,000/cmm.
- Child under 2 years = 6200 to 17,000/cmm.
- Newborn = 9000 to 30,000/cmm.
What is the differential count of peripheral blood?
| Type of the cells | % | Absolute count |
|
|
|
|
|
|
|
|
|
|
|
|
What are the causes of increased TLC (Leucocytosis)?
- The TLC is >11000/cmm.
- Mostly in the case of infections that may be bacterial or viral.
- Localized infections are:
- Meningitis.
- Pneumonia.
- Abscess.
- Tonsillitis.
- Generalized infections:
- Septicemia.
- Acute rheumatic fever.
- Cholera.
- Localized infections are:
- In the case of leukemias.
- After the strenuous exercise.
- Pain and anorexia.
- Epileptic seizures.
- Emotional reaction.
- Mild leucocytosis in pregnancy.
- Acute hemorrhage.
- Intoxications like:
- Poisoning by drugs, chemicals, and venoms (black widow spider).
- Metabolic diseases include uremia, acidosis, eclampsia, and acute gout.
- Parenteral proteins and vaccines.
- Acute hemolysis of red blood cells.
- Myeloproliferative diseases.
- Tissue necrosis:
- Burns.
- Gangrene.
- Necrosis of the tumor.
- Acute myocardial infarction.
- Necrosis due to bacteria.
- Physiologic conditions are:
- Emotional stress.
- Exercise.
- Obstetrical labor.
- Menstruation.
What are the causes of decreased leucocytosis (neutropenia)?
- The TLC is <4000/cmm.
- This may be seen in fever, malaise, and chills.
- Bacterial Infections:
- Bacterial.
- Septicemia.
- Miliary tuberculosis.
- Typhoid fever.
- Paratyphoid fever.
- Tularemia.
- Brucellosis.
- Viral infections are:
- Hepatitis.
- Influenza.
- Infectious mononucleosis.
- Psittacosis.
- Rubella.
- Measles.
- Hematological diseases:
- Aleukemic leukemia.
- Pernicious anemia.
- Gaucher’s disease.
- Felty’s syndrome.
- Aplastic anemia.
- Deficiency of vitamin B12.
- Drugs and chemicals:
- Antibiotics.
- Analgesics.
- Sulphonamides.
- Antithyroid drugs.
- Arsenicals.
- Marrow depressant.
- Malignant infiltration of the bone marrow.
- Bone marrow aplasia.
- Bone marrow depression by radiations.
- Autoimmune diseases like SLE.
TLC counted in Neubauer chamber:
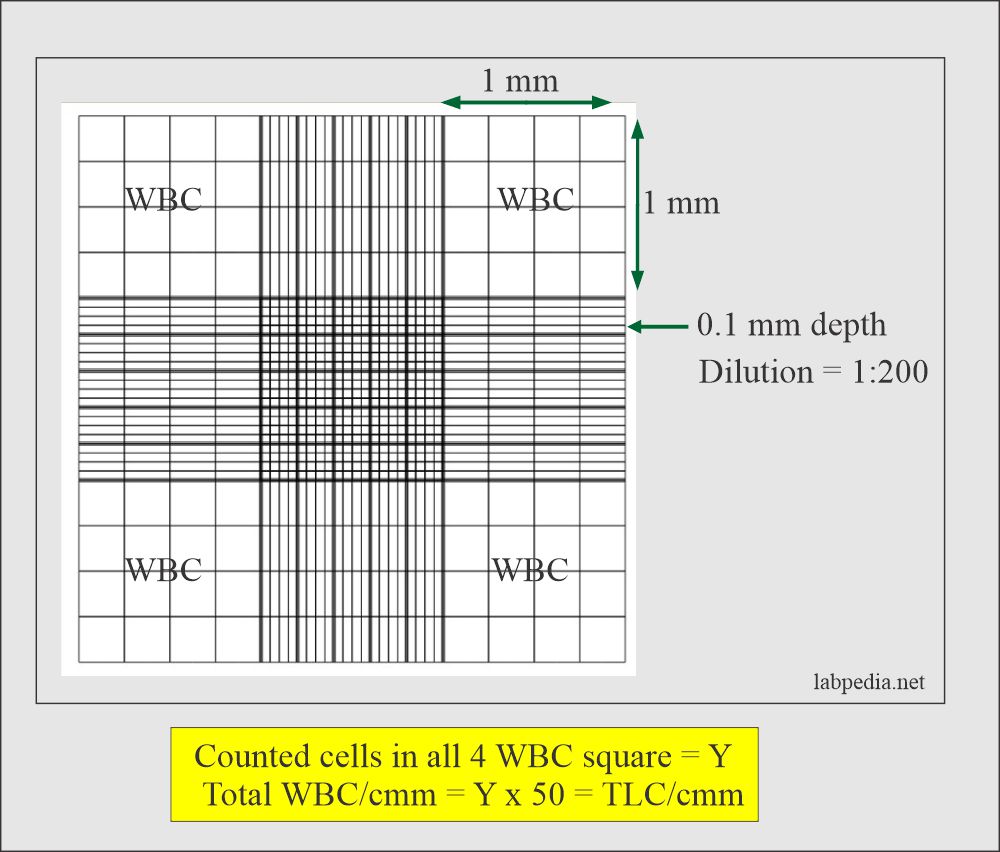
Neubauer chamber counting of white blood cells (TLC)
- Please always correlate TLC with the freshly prepared peripheral blood slide.
- Critical value = <2500 or >30,000 /cmm.
Questions and answers:
Question 1: Is there an effect of exercise on TLC?
Question 2: What is the target organ of IL-3?
- Please see more details in CBC part 1.