Spleen, Hypersplenism , Splenomegaly
Hypersplenism is characterized by a triad of :
- Splenomegaly
- There is a decreased number of RBCs, WBCs, Platelets or combination of these three elements.
- Above deficiency of the cells can be corrected by splenectomy.
Mechanism of hypersplenism:
- This is uncertain but there are postulates.
- This may be due to increased sequestration.
- This may be due to lysis of the cells by macrophagic cells.
Splenomegaly
Etiological classification
1. Infections: There is enlargement of the spleen in acute pyogenic infection. In septicemia, the spleen is enlarged and called septic spleen.
While non-pyogenic bacteria are Tuberculosis, Typhoid, Brucellosis, and Sarcoidosis.
BEST4 CMH KI
B = Brucellosis E = Echinococcus S = Syphilis and Subacute bacterial endocarditis T 4 = T.B, Typhoid, Toxoplasmosis and Trypanosomiasis
C = CMvirus M = Malaria H = Histoplasmosis K = Kala-azar I = Infectious mononucleosis.
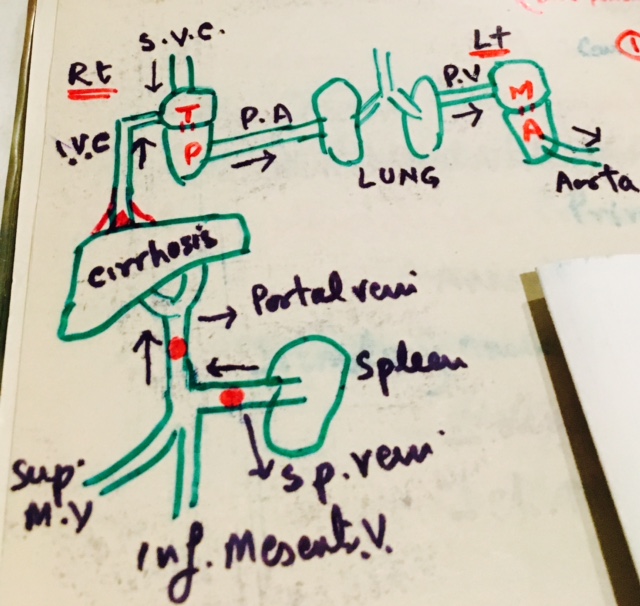
2. Circulatory disturbance: Persistent or chronic venous congestion leads to congestive splenomegaly. This is due to the portal or splenic vein hypertension.
- Right heart causes are a chronic congestive failure, Rarely the weight is more than 500 gram.
- Cirrhosis will lead to increased portal vein pressure due to fibrosis. Massive enlargement 1000 to 5000 grams.
- Portal vein or splenic vein thrombosis may be seen in pylephlebitis or in carcinoma of stomach and pancreas.
3. Storage diseases: This may be due to :
- Amyloidosis and it gives rise to Sago’s spleen.
- Lipid storage diseases are Familial hyperlipidemia like:
- Deficiency of alpha-lipoprotein.
- Poorly controlled diabetes.
- Hypothyroidism.
- Prolonged obstructive jaundice.
Hereditary causes are :
- Gaucher’s disease.
- Niemann Pick disease.
- Glycogen storage disease.
4. Neoplasm :
- Primary causes are rare benign tumors like Fibroma, Osteoma, Chondroma, and cyst.
- Primary malignant tumors are Non-Hodgkin’s lymphoma and Hodgkin’s lymphoma.
- Secondary tumors are lymphomas and rarely carcinoma and sarcoma.
5. Blood disorders :
- Primary causes lead to anemia, thrombocytopenia, and leucopenia.
- Secondary causes are hemolytic anemia, Idiopathic thrombocytopenia (ITP), leukemia and lymphoma infiltrate, chronic marrow failure like myeloid metaplasia.
6. Immunological conditions like Rheumatoid arthritis and systemic lupus erythematosus (SLE).
7. Splenic infarct in early-stage leads enlargement of the spleen. Later on, fibrosis may bring it back to normal size.
Causes are :
- Occlusion of a major splenic artery or branch due to emboli from the heart.
- Septic infarct in infective endocarditis.
- The Less common cause is local thrombosis in myeloproliferative disorders and sickle cell anemia.