Chapter 25: Autoimmune diseases – Rheumatic Fever
January 12, 2021Elementary Immunology
RHEUMATIC FEVER
Definition
- Rhematic fever is an autoimmune systemic disease due to cross-reactivity with Group A β-hemolytic streptococci, usually after the throat infection.
- In susceptible persons, around 2% of the population shows permanent damage to the heart valves.
Rheumatic Fever may be:-
- A. Acute rheumatic fever indicates acute illness. This is the disease of childhood.
- B. Chronic rheumatic disease refers to chronic heart disease.
- C. Rheumatic heart disease is a disease of adulthood. It is seen at an average age of 25 to 34 years.
Age
- This is a disease of children.
- Peak age is 5 to 15 years.
Incidence
- This disease is common in the third world and rare in developed countries.
- This disease follows the latent period of 2 to 4 weeks.
Evidence of streptococcal infection:
- History of scarlet fever.
- Positive growth from throat on culture.
- If there is an increase in the ASO titer (anti-streptolysin O antigen).
- To qualify for rheumatic fever, one of the above is enough.
Signs and symptoms of Rheumatic fever:
- There is a fever.
- Majority show polyarthritis of larger joints.
- There may be carditis. There is permanent damage to the heart valves, and also there is an increased risk for future endocarditis.
- Mitral regurgitation is the early predominant findings.
- Mitral stenosis progressively becomes more common with increasing age.
- There is a nodule called Aschoff’s Bodies. These consist of necrosis, pleomorphic cellular infiltrate, and Aschoff’s Cells.
- These are found in the heart and more prominent in the myocardium. Aschoff giant cell is multinucleated giant cells.
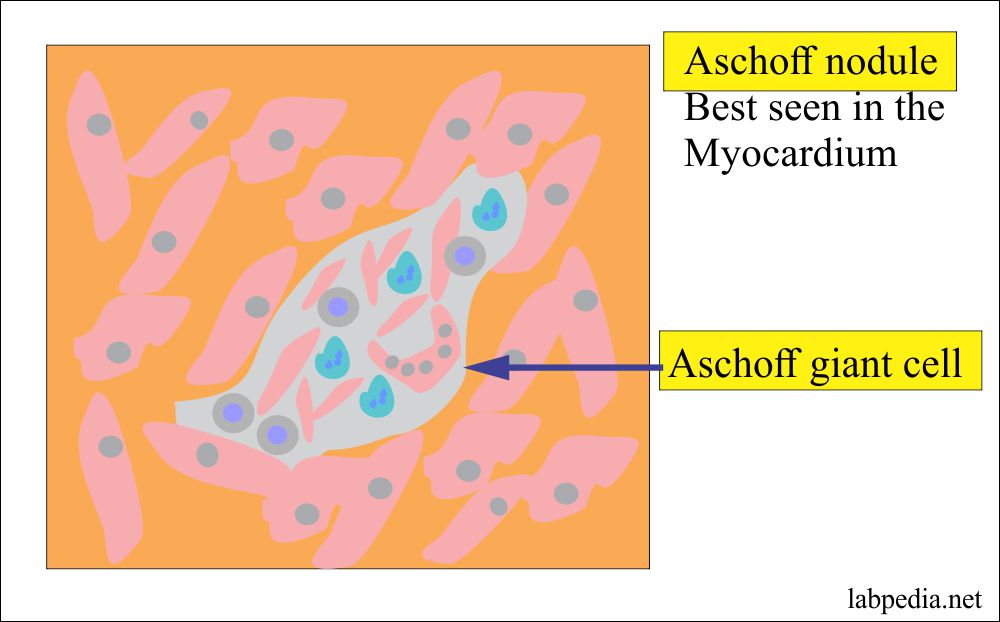
Rheumatoid fever Aschoff nodule
- These are found in the heart and more prominent in the myocardium. Aschoff giant cell is multinucleated giant cells.
- There is an erythema marginatum of the skin.
- Scarlet fever:
- This is the result of pharyngeal infection by streptococcal group A (β-hemolyticus).
- This organism produces erythrogenic toxins, which lead to a characteristic rash.
- Scarlet fever S/S are streptococcal pharyngitis and characteristic skin rash.
- The patient may show Sydenham’s chorea.
- It usually follows H/O pharyngitis due to streptococcus group A, which appears after 3 weeks of infection.
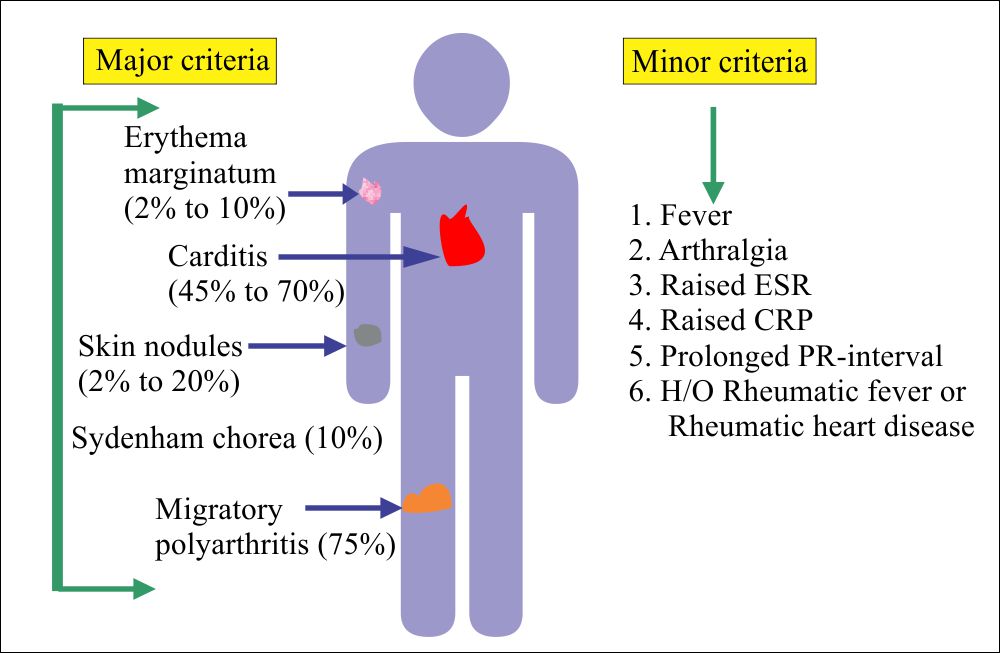
- Major criteria for Rheumatic fever are:
- WHO modified these criteria.
- Recent evidence of streptococcal infection or scarlet fever.
- No need for infection in the case of either carditis or chorea.
- Apple the Jones criteria.
- Patient with Rheumatic heart disease needs only two minor criteria.
- Carditis in various forms is seen in 45% to 70%.
- Migratory polyarthritis, seen in 75% of the cases.
- Sydenham’s chorea is seen in 10% of the cases.
- This is characterized by:
- Rapid, irregular, and aimless movements.
- These movements are seen in arms, legs, trunks, and facial muscles.
- Subcutaneous skin nodules are seen in 2% to 20%.
- Erythema marginatum is seen in 2% to 10%. These are the skin rashes present on the trunk and limbs.
- WHO modified these criteria.
- Minor criteria for Rheumatic fever are:
- There is raised ESR.
- There is an increase in the C-reactive protein (CRP).
- There may be a fever.
- There is a prolonged P-R interval.
- There may be previous H/O of rheumatic fever or rheumatic heart disease.
Rheumatic fever diagnostic criteria
Jones Revised criteria for the diagnosis of Rheumatic fever:
Major Criteria Minor criteria Streptococcal infection evidence Carditis (45% to 70%) Raised ESR Positive throat culture Polyarthritis (75%) Raised and positive CRP The increasing titer of ASO Skin nodules (2% to 20%) Fever Sydenham chorea (10%) Prolonged PR interval Erythema mrginatum (2% to 10%) H/O Rheumatic fever or RHD Arthralgia
- Rheumatic fever = 2 major criteria or One major + 2 minor criteria
Etiology and Pathogenesis
- Direct infection: – But this possibility is ruled out because the lesion is sterile.
- This may be due to streptococcal toxins. Streptolysin-SS is not immunogenic. Streptolysin-SO is immunogenic, and it may form Anti-SO Ab, which forms (SO + Anti-SO) immune complexes. Myocardium competes for Ig, and these complexes deposit there.
- Streptolysin O (SO) is an extractable toxin with hemolytic properties produced by the group A β- hemolytic streptococci.
- In the tissue, this SO antigen produces antibody ASO (antistreptolysin antibody).
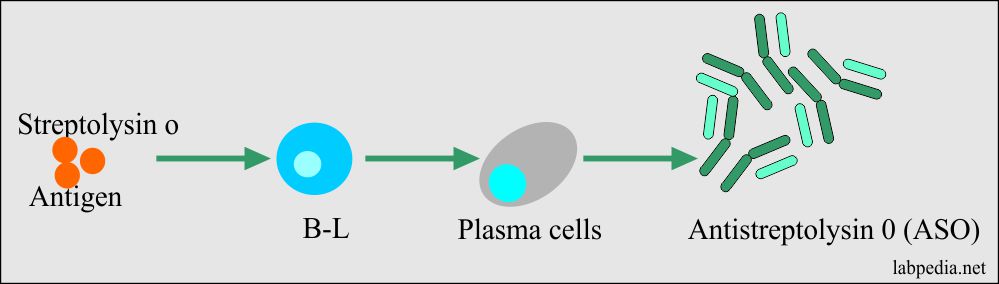
Formation of ASO antibodies
- Cross-reacting Ab: – The antibody against streptococcal M-protein may cross-react with cardiac muscles.
Mechanism of Injury
- It is a type III immune-complex disease.

Rheumatic fever mechanism of injury to the tissues
Pathology
- In some cases, only the kidney is involved. It starts as acute and becomes a chronic disease.
- The earlier lesion is Aschoff’s Body. These are seen in the interstitium of the myocardium close to coronary arteries. Mitral and aortic valves are commonly involved. The cause of heart failure in acute cases is not known.
- In some cases, lungs may be involved, and patients may develop pleurisy.
- Arthritis does not cause crippling disease in the patient.
- In the kidney, there is diffuse proliferative glomerulonephritis occasionally with crescent formation.
- The complication of rheumatic fever is chronic heart disease and poststreptococcal glomerulonephritis.
Diagnosis
- There is a history of streptococcal infection (Sore-throat).
- Raised antistreptolysin O level (ASO). This antibody will detect:
- Rheumatic fever.
- Glomerulonephritis.
- Endocarditis.
- Scarlet fever.
- Titers of ASO will be raised. A rising titer is more important than a single titer.
- Its low concentration may be seen in normal children.
- Normal ASO titer = <160 Todd units (<200 IU).
- The titer of 160 Todd units is definitely raised level.
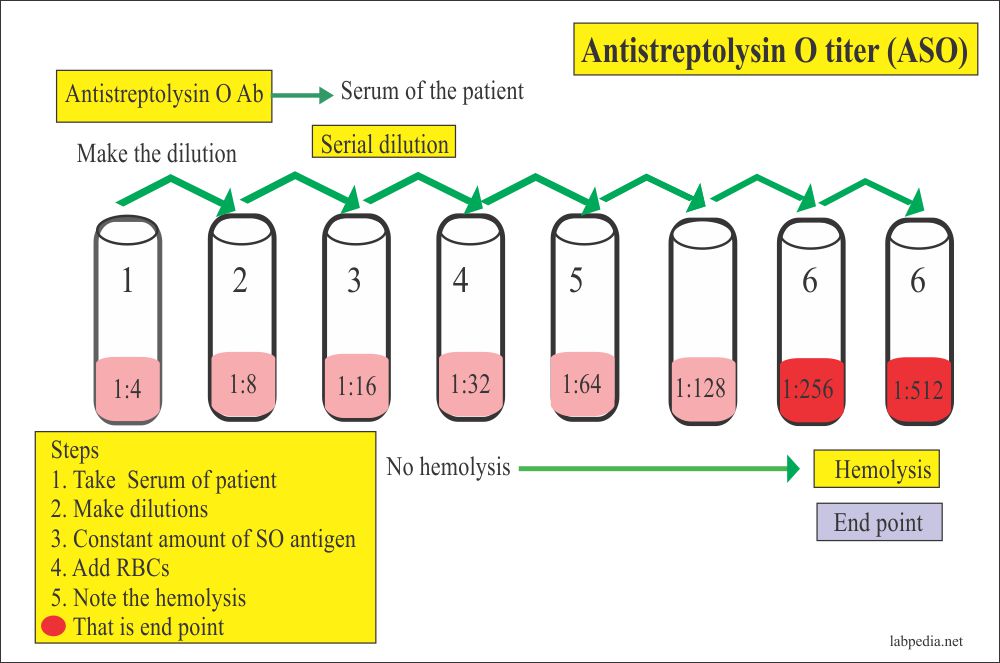
Procedure for ASO titer
- There is a leucocytosis.
- There is typically raised ESR and CRP positive.
Treatment
- Patients must do rest until CRP level is normal for at least.
- Injection penicillin is given.
- For arthritis and cardititis give analgesics.
- In case of severe joint pain, it can immobilize the joints.
- Haloperidol is given in the case of Sydenham’s chorea.
The outcome of the Rheumatic fever:
- The average acute attack lasts for 3 months.
- Recurrent attacks are possible in case of reinfection with streptococci, pregnancy, and contraceptive pills.
- 60% of the cases with carditis develop chronic rheumatic heart disease.
- Involvement of the valves is mitral (70%), aortic (40%), tricuspid (10%), and pulmonary (2%).
Prophylaxis:
- After the Rheumatic fever, give an injection of penicillin V until the patient is 25 years old.
- Give antibiotics for the dental or other operative procedures.