Chapter 22: Autoimmune diseases, Pernicious Anemia (Vitamin B12 Deficiency)
PERNICIOUS ANAEMIA (PA)
Definition
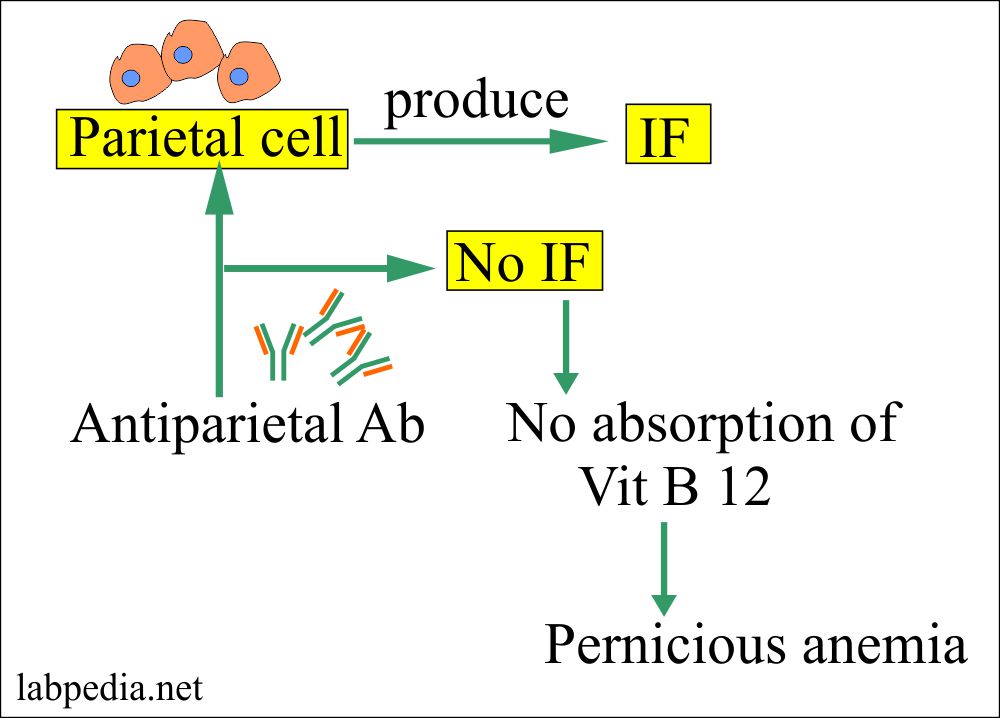
This is megaloblastic anemia due to deficiency of vitamin B12, because of malabsorption, which is believed as an autoimmune phenomenon to gastric parietal cells and their products.
Parietal cells are the source of intrinsic factor. This intrinsic factor binds the B12 and allows its absorption in the ileum.
Pernicious anemia, the role of parietal cells
Age and Sex
PA is more common in a temperate climate. It affects both sexes equally. It is rare under the age of 30; the average presenting age is 60 years.
Source of vitamin B12
Vitamin B12 is supplied in the diet and it is present in:
- Meat.
- Eggs.
- Dairy products.
Signs and Symptoms
- The patient is pale and slightly jaundiced.
- Gastrointestinal manifestations are a result of vitamin B12 deficiency like a sore tongue, which appears as beef red.
- Neurological manifestations are serious. The patient may have paraesthesia, numbness, and ataxia.
- There is a dietary deficiency in:
- Pregnancy.
- Tapeworms infestation (Diphyllobothrium latum).
- Intestinal resection particularly ileum.
- Malabsorption syndrome.
- There may be:
- There may lemon tinge on the skin.
- There may be retinal hemorrhage.
- Patients may have a fever but this is rare.
- There may be splenomegaly.
- Patients may develop retrobulbar neuritis.
Common clinical features are:
| Clinical features | Possible percentage |
| Fatigue and weakness | 90% |
| Dyspnoea | 70% |
| Paresthesia | 38% |
| Sore, red tongue | 25% |
| Diarrhea | Rare |
| Dementia | Rare |
| Antibodies to parietal cells | 90% |
Microscopy
Gastric biopsy Shows gastric atrophy affecting the acid and pepsin-secreting portion of the stomach and the antrum is unaffected.
Pathogenesis
- The parietal cells of the gastric mucosa in the fundal area produce an intrinsic factor for the absorption of vitamin B12 and HCL for the absorption of iron.
- The intrinsic factor is a glycoprotein.
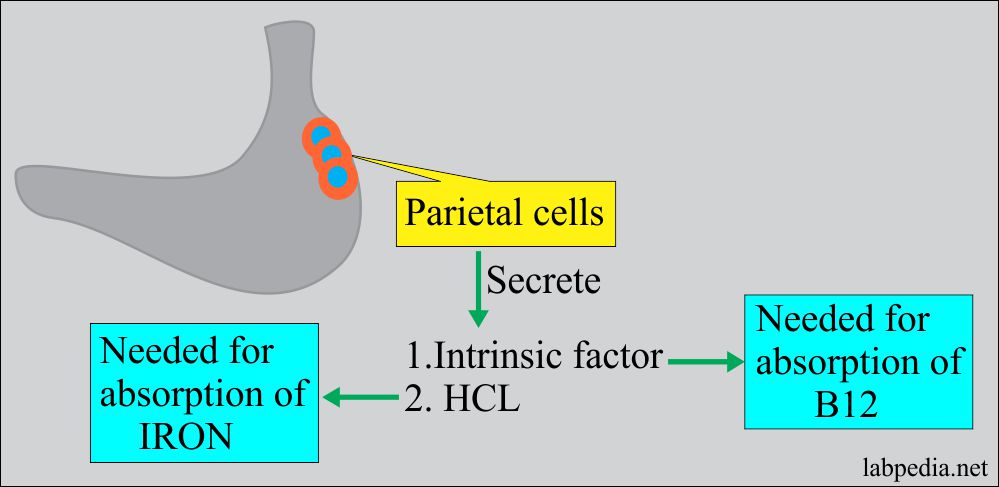
Pernicious anemia and role of parietal cells
- Cobalamine combine with an Intrinsic factor in the stomach in an acid medium.
- In the stomach, it splits from the dietary proteins and forms the complex IF+B12.
- In the ileum, this complex attaches to the receptor of the microvillous cells.
- Transcobalamin II (TC II) is synthesized in the liver and it carries B12 (TCII+B12).
- This (TC II+B12) complex carried to other tissue and liver.
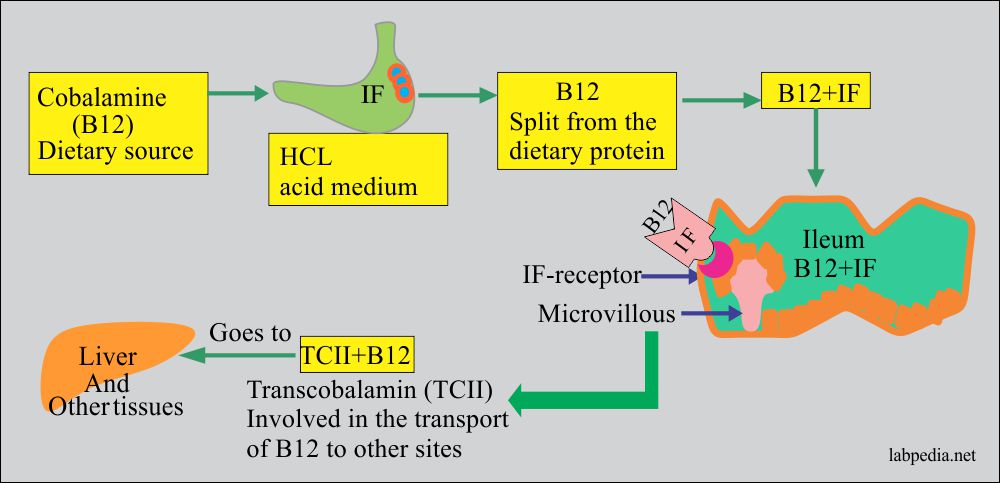
Pernicious anemia, absorption of the B12
- Atrophic gastritis is usually present, .
- In B12 deficiency, synthesis of thymidine is affected, hence DNA formation is impaired, and as a result RBCs production is decreased.
- Pernicious anemia results from the destruction of the gastric parietal cells, with subsequent loss of intrinsic factor which leads to an inability to absorb vitamin B 12.
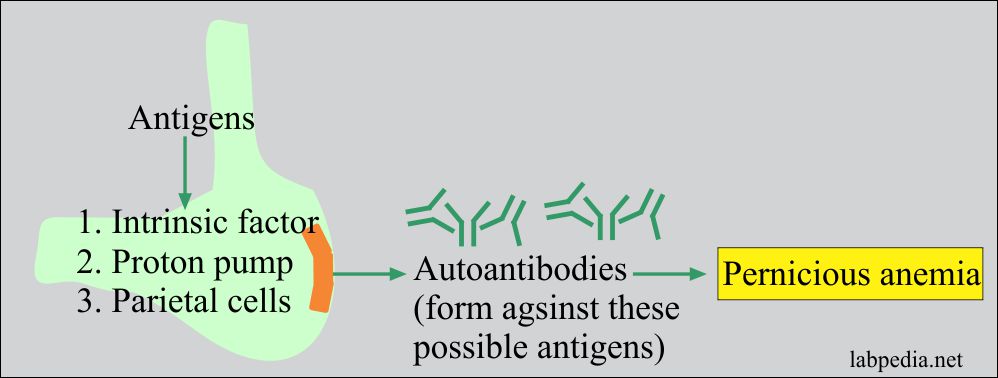
Pernicious anemia antigens
- There are autoantibodies against:
- There is gastric parietal cell antigen which gives rise to autoantibodies, virtually present in all patients. These are present in 20 to 30% of first-degree relatives and 5% in the normal population.
- There are autoantibodies against the proton pump that will acidify the stomach lumen contents. Acidity is important for the release of B12 from the salivary gland proteins.
- Autoantibody against intrinsic factor (IF) is of two types, one is blocking, and the second is a binding antibody:
- Blocking autoantibody reacts with the combining site for vitamin B12 on the intrinsic factor (IF) and is found in most patients (>70%).
- Binding autoantibody reacts with another epitope on the intrinsic factor (IF).
- The presence of antibodies against the B12 binding site on intrinsic factor strongly indicate pernicious anemia.

Fig 147: Pernicious Anemia Mechanism
Diagnosis
- Peripheral blood shows macrocytosis (MCV > 100ft).
- Hb = 3 to 11 g/dL.
- RBC count = Decreased.
- MCV = >110 fl.
- Mild neutropenia.
- Mild thrombocytopenia.
- Serum iron is increased.
- Total iron-binding capacity is normal or decreased.
- Serum ferritin is increased.
- % of iron saturation is increased.
- The reticulocyte count is low.
- Neutrophils are typically hypersegmented.
- Bone marrow is hypercellular and decreased myeloid: erythroid ratio. RBC precursors are large with immature nuclear morphology.
- The presence of IF-blocking antibodies is diagnostic.
- 80% of patients have parietal cell antibodies.
- Vitamin B12 estimation will show a deficiency. This is below 90 pg/mL.
- When there is B12 deficiency then folate level will be normal.
- Schilling test will confirm the diagnosis.
- This test finds the ability of the patient to absorb B12 first without, and then with, a dose of exogenous intrinsic factor.
- Radiolabeled B12 is ingested, and the 24 hours urine sample is collected.
- If >7% of the radiolabeled material excreted in the urine, it means absorption is normal.
- If <7% of the radiolabeled material excreted in the urine, it means absorption is abnormal.
- In case of the abnormal result:
- Repeat the test with the addition of an intrinsic factor.
- If absorption corrects, this favors the deficiency of the endogenous intrinsic factor as seen in pernicious anemia.
- If it does not correct, then the possibility is intestinal malabsorption which causes B12 deficiency.
Treatment
Vit-B12 replacement therapy corrects all but not the neurological abnormalities.
Complication
Patients with PA develop gastric polyp very frequently and there are more chances to develop malignant tumors of the stomach.
Prognosis
- Complete neurological recovery is possible.
- Patients respond if treated in 3 to 6 months of onset. Early treatment is recommended.
I would like to add a Note asking you about your view on what I have read in PDQ Haematology Book:
“The degree to which the neurologic disease is reversible is variable and difficult to predict. Neurologic symptoms of recent onset (within a few months) are likely to be completely reversible. Abnormalities that have been present for 6 months or more are likely to result in permanent residual deficits. It usually takes 6 months or longer to achieve maximum benefit; however, some patients continue to show neurologic improvement up to 1 year.”