ASO Titer (Antistreptolysin O titer)
Antistreptolysin O titer (ASO)
What sample is needed for the Antistreptolysin O titer (ASO)?
- The test is performed on the patient’s serum (clotted blood, 3-5 mL).
- A random sample can be taken.
- Avoid hemolysis.
What are the Indications for the Antistreptolysin O titer (ASO)?
- To diagnose exposure to Streptococcal infection.
- To diagnose poststreptococcal diseases, such as:
- Glomerulonephritis.
- Rheumatic fever.
- Bacterial Endocarditis.
- Scarlet fever.
- A significant level was seen in glomerulonephritis and rheumatic fever.
What are the precautions for the Antistreptolysin O titer (ASO)?
- Avoid the drug-like steroids and antibiotics that decrease the ASO titer.
- Increased beta-lipoprotein inhibits streptolysin O and gives a falsely high ASO titer.
- Early injection of penicillin prevents the rise of the titer.
What are the complications of Streptococcus group A?
- Lancefield group A streptococci are also known as Streptococcus pyogenes.
- Group A β-streptococci produce various infections; the most common is acute pharyngitis.
- It can produce scarlet fever, erysipelas, vesicular cellulitis, and puerperal fever.
- There are a few reports showing conditions like staphylococcal toxic shock syndrome.
What enzymes are produced by the Beta-hemolytic Streptococci group A?
- Beta-hemolytic group A streptococci produce many enzymes that can contribute to their pathogenicity. Two of these are:
-
Streptolysin O:
- O stands for oxygen-labile, as it is inactivated by oxygen.
- Streptolysin O is produced after 7 to 10 days of the infection, and antibodies start to appear.
- At the end of 2 months, only 70% to 75% of the tests are positive.
- At 6 months, 35% of the cases are positive.
- At 12 months, 20% are positive.

ASO and SO titer interpretations
-
- What are the functions of Streptolysin O?
- Streptolysin O enzyme destroys the red blood cells and white blood cells.
- This is why it is called β-hemolytic group A streptococci and exhibits beta-hemolytic activity.
- This enzyme is antigenic.
- Patients develop an anti-streptolysin O (ASO) antibody.
- The highest level of ASO titer occurs during the third week of infection for acute rheumatic fever.
- At this stage, positivity is 80% to 85%, and antibodies start declining later.
-
Streptolysin S:
- The “S” stands for oxygen stable.
- This can cause beta hemolysis.
- This is not antigenic.
How will you determine Antistreptolysin O (ASO)?
- ASO is measured by the latex agglutination or haemagglutination procedure.
- This test measures antibodies against Streptolysin O, an antigen produced by Group A beta-hemolytic streptococci.
- RBCs are added as an indicator system.

ASO causing hemolysis
- The ASO antibody may be detected in the blood weeks or months after the infection has resolved.
What are the important facts about Beta-Streptococci?
- Group A-beta streptococci can be isolated from throat or nasopharynx culture in 15% to 20% (range 11% to 60%) of normal children.
- Taking two swabs instead of one will increase the likelihood of a positive culture result.
- Group A streptococci are always sensitive to penicillin, as confirmed by in vitro sensitivity testing.
- Streptolysin O is an extracellular toxin produced by many of the streptococci groups, particularly by group A β-hemolytic streptococci.
- Streptolysin O has the ability to destroy the red blood cells (hemolysis).
- The Streptolysin O enzyme is antigenic, and the immune system produces antibodies, such as the Antistreptolysin O antibody (ASO).

ASO antibody formation
When is the time of the appearance of ASO and SO?
- SO is antigenic, and it produces an antibody against the SO antigen.
- ASO appears in the serum approximately one week to one month after a streptococcal infection.
- This ASO is a neutralizing antibody.
- ASO has no value for the diagnosis of acute streptococcal infection.
- The rising serial titer of ASO over weeks, followed by a gradual decline in titer, is more significant for streptococcal infections.
- After 6 months, only 30% of the patients show abnormal titer.
- The highest level of ASO is seen in glomerulonephritis and rheumatic fever.
- A fourfold rise in the titer is significant for acute and convalescent patients.
- The 500 to 5000 Todd units/mL level suggests acute post-streptococcal glomerulonephritis, rheumatic fever, or acute poststreptococcal endocarditis.
- 15% of the active Rheumatic fever patients show a test negative.
What is the procedure for the Antistreptolysin O titer (ASO) antibody titer?
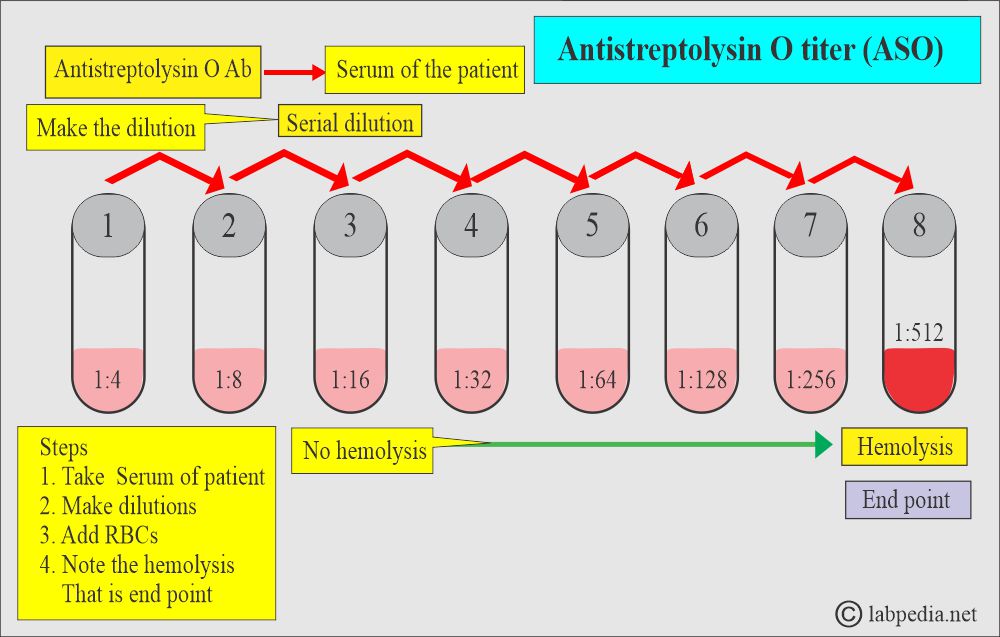
ASO titer procedure
What is the interpretation of the ASO titer?
- The rising titer is more significant than a single test.
- It is positive when it is >250 IU. Positive levels are from 400 to 5000 IU.
- ASO, even in streptococcal infections, is elevated in 70% to 80% of patients.
- The raised level of the ASO is not related to the severity of the disease, and the fall is also unrelated to the disease’s course.
- Approximately 30% to 40% of patients with streptococcal pyoderma exhibit elevated ASO levels.
- 50% of patients show raised ASO levels in glomerulonephritis, and 20% is seen in membranous glomerulonephritis.
What is the value of Antistreptolysin O (ASO) titer in various diseases?
| Clinical condition | ASO level in Todd units |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Where will you see False-positive results?
- Patients with tuberculosis.
- Liver diseases like active viral hepatitis.
- Bacterial contamination.
- The latex agglutination test may yield a false-positive result in samples with lipemia or contamination.
What is the normal antistreptolysin O (ASO)?
Source 2
- Adult / elderly =>160 Todd unit/mL or <200 IU.
- 6 months to 2 years = ≤50 Todd units/mL.
- 2 to 4 years = ≤ 160 Todd units /mL
- 5 to 12 years = 170 to 330 Todd units/mL.
- If it is >200 Todd units, then it is a significant level; it suggests recent or relatively recent group A streptococcal infection.
- A greater than 500 Todd units indicates acute rheumatic fever or acute post-streptococcal glomerulonephritis.
- Serial assay of ASO should be advised for rising titer.
What direct evidence of antistreptococcal antibodies indicates?
- Streptococcal pharyngitis and tonsillitis.
- Scarlet fever.
- Erysipelas.
What is the indirect evidence of ASO for the diagnosis of?
- Rheumatic fever.
- Differential diagnosis of joint pains of rheumatoid arthritis and rheumatic fever.
- Detection of the subclinical streptococcal infection.
- Glomerulonephritis.
What is the relation between Streptococcal infections and ASO titer?
- An ASO titer raised above the baseline indicates recent group A streptococcus pharyngitis within the last 2 months.
- The increased titer develops 7 to 14 days after infection and rises rapidly to a peak within 4 to 6 weeks.
- Then it declines in the next 4 to 6 months.

ASO values in active infection
What are the causes of a raised ASO titer?
- Bacterial Endocarditis.
- Post-streptococcal glomerulonephritis (50% to 70 % of the patients show no high titer).
- Rheumatic fever.
- Scarlet fever.
- Streptococcal pyoderma.
- ASO is often not raised in these diseases.
What is important for the ASO titer?
- An increased titer may be found in the healthy carrier.
- Antibiotic therapy may suppress the antibody response.
- Increased Lipoprotein levels inhibit Streptolysin O and produce a falsely high ASO titer.
Questions and answers:
Question 1: What is the value of ASO for the active stage of Rheumatic fever?
Question 2: Can we see ASO in normal people?